It began, as many federal investigations do, with a whisper—an anomaly buried deep within a sea of billing records. A pattern too consistent to be random. A number too large to ignore. What followed would unravel into one of the most disturbing healthcare fraud cases in recent California history, exposing a system where compassion had been meticulously repurposed into a multimillion-dollar enterprise.
Federal agents moved quietly at first. Subpoenas were issued. Financial trails were mapped. Patient records—thousands of them—were reviewed with clinical precision. What they found was not negligence or oversight. It was something far more calculated.
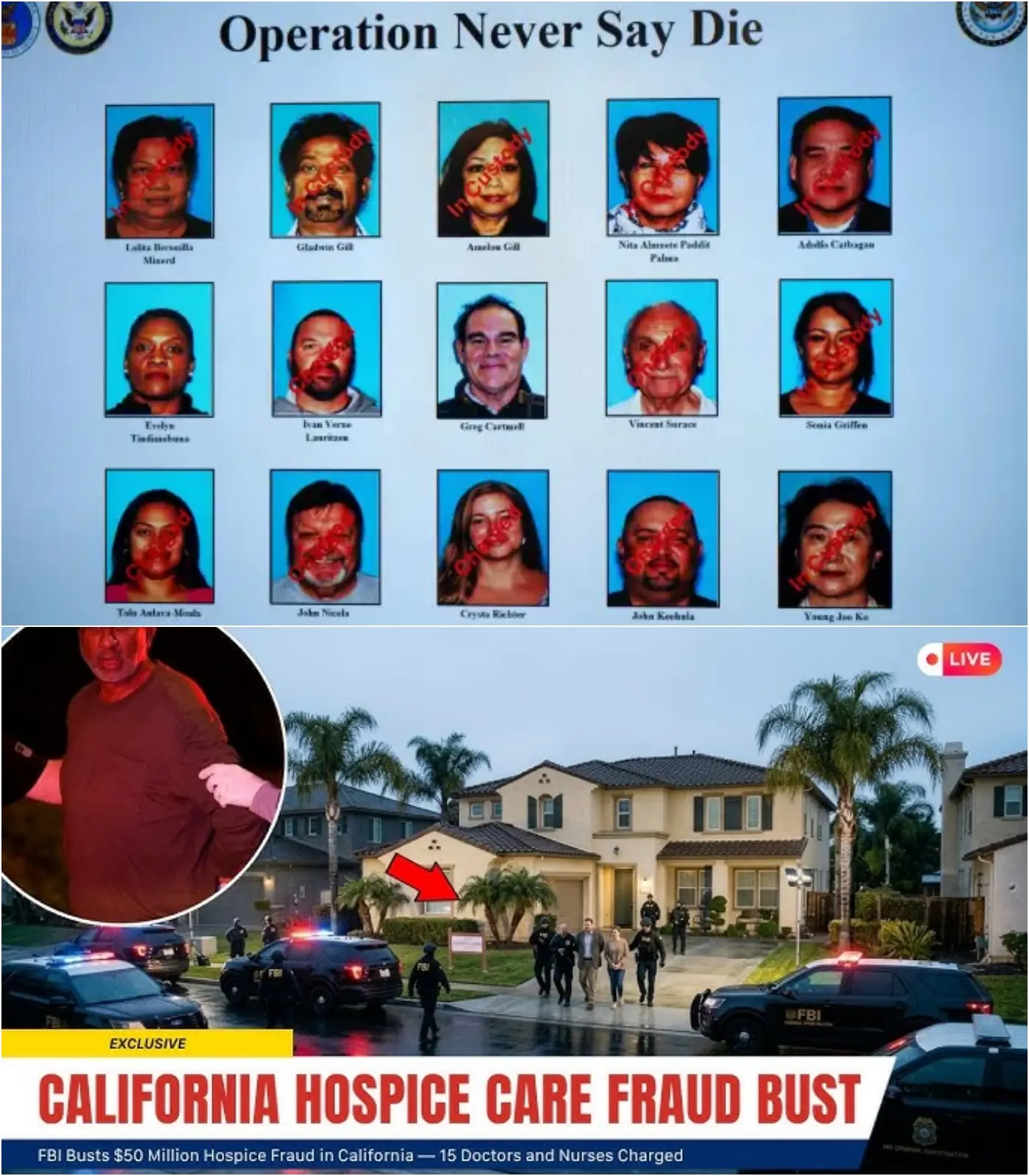
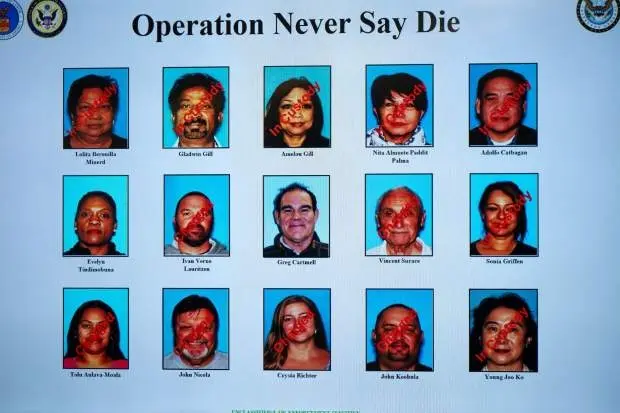
According to federal authorities, a sprawling network of 15 licensed medical professionals—doctors and nurses entrusted with end-of-life care—now stands accused of orchestrating a $50 million hospice fraud scheme. The charges paint a chilling picture: vulnerable patients allegedly enrolled into hospice care without proper medical justification, their final days transformed into revenue streams.
Hospice care, by design, is meant for those nearing the end of life—a space where dignity replaces aggressive treatment, where comfort becomes the priority. It is, perhaps, one of the most sacred corners of modern medicine. But in this case, investigators allege, that sacred trust was systematically exploited.
The scheme, officials say, operated in plain sight.
Patients—many of them elderly, some with manageable or non-terminal conditions—were allegedly recruited into hospice programs under false pretenses. In some cases, families were misled. In others, they were never fully informed of what hospice enrollment truly meant. Once enrolled, these patients generated steady streams of Medicare reimbursements, often reaching thousands of dollars per month per individual.
Behind closed doors, the machinery of fraud churned on.
Medical certifications were allegedly falsified to meet hospice eligibility criteria. Diagnoses were exaggerated. Prognoses were manipulated. Nurses and physicians, bound by oath to do no harm, are now accused of signing off on documents that turned routine care into lucrative deception.
The financial scale alone is staggering—$50 million siphoned through a system designed to care for the dying. But for investigators, the deeper concern lies not just in the money, but in the human cost.
“This wasn’t just fraud. It was a betrayal,” one federal official familiar with the case said, speaking under condition of anonymity. “These are patients at their most vulnerable. Families placing trust in professionals during incredibly emotional moments. That trust was weaponized.”
As the investigation unfolded, agents reportedly uncovered a complex web of shell companies, referral networks, and financial kickbacks. Hospice providers allegedly paid recruiters to identify and funnel patients into the system. In some instances, these recruiters targeted specific communities, zeroing in on individuals who might be less likely to question medical authority.
The homes tied to the accused professionals tell a quieter, more unsettling story. Neatly trimmed lawns. Quiet suburban streets. The kind of places where neighbors wave politely but rarely ask questions. It is within these ordinary settings, investigators allege, that extraordinary deception was planned and executed.
For years.
The charges filed this week mark a significant escalation in the federal government’s effort to combat healthcare fraud, particularly within hospice services—a sector that has seen explosive growth in recent years. With that growth, experts warn, comes increased risk.
Oversight mechanisms, while robust on paper, often struggle to keep pace with the complexity of modern fraud schemes. Billing systems can be manipulated. Documentation can be fabricated. And when multiple professionals collaborate, the illusion of legitimacy becomes harder to pierce.
“This case highlights systemic vulnerabilities,” said a healthcare policy analyst who has followed hospice industry trends for over a decade. “When financial incentives are tied so directly to patient enrollment, it creates opportunities for abuse—especially if oversight isn’t aggressive and continuous.”
Yet for many families, the revelations are more than policy concerns. They are deeply personal.
Some are now questioning whether their loved ones were unnecessarily placed into hospice care. Others wonder if critical treatments were delayed or withheld because of decisions made under false medical pretenses. The emotional toll, much like the financial damage, continues to unfold.
Federal prosecutors have made it clear: this is not the end.
Additional investigations are reportedly ongoing, with authorities examining whether the network extends beyond the 15 individuals currently charged. There are also indications that more healthcare providers could come under scrutiny in the coming months.
Meanwhile, the accused face a series of serious federal charges, including healthcare fraud, conspiracy, and in some cases, identity theft. If convicted, they could face decades in prison, along with substantial financial penalties.
But beyond the courtroom, the case has ignited a broader conversation—one that cuts to the core of trust in the healthcare system.
How did this go undetected for so long? Were warning signs missed—or ignored? And most importantly, how can such a breach of trust be prevented in the future?
Regulators are now under increasing pressure to tighten oversight, implement more rigorous auditing systems, and ensure that hospice eligibility criteria are enforced with greater scrutiny. Lawmakers, too, are beginning to take notice, with calls for reform gaining momentum.
Yet even as policy debates unfold, one truth remains unavoidable: systems are only as strong as the people within them.
In this case, investigators allege, those entrusted with care chose exploitation instead.
The image is difficult to reconcile—a physician signing off on a terminal diagnosis that may not exist, a nurse documenting decline where there is stability, a network profiting not from healing, but from the illusion of it.
And somewhere in the middle of it all are the patients—individuals who believed they were receiving compassion at the end of life, unaware that their care may have been part of something far more calculated.
For federal agents, the work continues. For families, the questions linger. And for the healthcare system, the reckoning may just be beginning.
Because when trust becomes currency, and care becomes a transaction, the cost is measured in more than dollars.
It is measured in dignity. In integrity. And in the quiet, irreversible moments that define the end of a life.